Nearly all young people who die of drug overdose begin their drug use with marijuana. A national policy based on harm reduction will never be nearly as effective as a policy based on drug prevention. We support addiction treatment, but admit there is no guarantee of success.
Yesterday a coalition of national groups ran an ad in the Washington Timescalling for enforcement of federal marijuana laws, as a step to end the national crisis of drug overdose deaths. The ad was sponsored by the National Institute of Citizen Anti-drug Policy (NICAP) Below is most of the full page ad:
By Robert L. DuPont, MD,President, Institute of Behavior and Health, a 501(c)3 non-profit organization working to reduce illegal drug use through the power of good ideas.
Often overlooked in discussions of drug policy today is the nature of the drug problem. The global drug problem can be traced to the innate nature of the human brain. The mammalian brain is extremely vulnerable to chemicals that stimulate brain reward. These chemicals are drugs of abuse. They produce far more intense brain reward than any natural reward, even sex and food. The repeated use of drugs of abuse leads to addiction. In its definition of addiction, the American Society of Addiction Medicine notes that it is “characterized by inability to consistently abstain, impairment in behavioral control, craving, diminished recognition of significant problems with one’s behaviors and interpersonal relationships, and a dysfunctional emotional response.”
Addiction is a chronic, often fatal, illness that typically begins in adolescence. The earlier an individual uses drugs of abuse, including alcohol and marijuana, the more likely it is that the person will develop a substance use disorder later in life. The best way to prevent addiction is to prevent the use of these substances. As a 13-year-old said to me years ago, “I don’t want to try cigarettes because I might like them.”
Modern Drug Use Epidemic
While the biology of addiction has not changed for millions of years, over the past half century drug use has changed dramatically. In the modern drug abuse epidemic, whole populations are exposed to a mind-bending array of drugs of abuse by powerful routes of administration. This has never happened before in human history.
Marijuana, the most widely used illegal drug, has been transformed in the time since the peak of its use in the United States in 1978. The potency of marijuana, as measured by the level of THC (the primary active cannabinoid in marijuana), has tripled over this time. New modes of marijuana consumption have increased the potency of marijuana delivery. For example, butane hash oil contains dramatically higher levels of THC, with concentrations up to 90 percent.
The addiction landscape also has changed as a result of the non-medical use of legal prescription drugs. Eighty percent of the global opioid supply is consumed by Americans who constitute less than five percent of the world’s population. With widespread medical use of opioid analgesics has come an epidemic of opiate dependence. The number of drug overdose deaths in the US has surpassed highway fatalities. The widespread use of prescription drugs has led to changes in the demographics of heroin use and subsequent heroin overdoses. Forty years ago heroin addiction was mostly confined to young inner-city men who often were involved in criminal activities. The new demography of heroin is the result of the demography of those that use pain medications non-medically. An estimated half of young heroin users previously abused prescription opioids prior to their heroin use. Heroin addiction has reached all parts of the country, especially small towns and rural areas, and is no longer limited to minority, male or lower income populations.
The drug epidemic continues to evolve in complex ways even as the public attitudes toward the use of drugs are shifting. Attitudes today are far more permissive toward the “recreational” use of drugs, especially marijuana. National polls indicate that a growing majority of Americans now favor legalization of marijuana for “recreational” use by adults.
Well-Funded Lobby Pushes for Marijuana Normalization
The well-funded lobby promoting the normalization of the use of marijuana (and other drugs) is based on the erroneous premise that marijuana is not only safe but also beneficial. (Ed. note: Three billionaires have spent an estimated $200,000,000 to legalize marijuana.) In contrast to this view, the science is clear that marijuana use is a serious threat to health, safety and productivity. As the negative impact of legal marijuana in the states of Colorado and Washington – and in the states that permit “medical” marijuana – is more widely understood, attitudes toward permissive drug use will shift once again.
The US, and the entire world, is at a crossroads in drug policy today with two oppositional perspectives on the future of drug policy. On the one hand is the vision on which current global drug policy was established in the first decades of the 20th century with the US in the lead which separates medical use from non-medical use of drugs with abuse potential. Under this framework, the goal of drug policy is to limit the use of drugs of abuse to medical uses only. Drugs of abuse are provided only through the process of physicians’ prescriptions and dispensed at pharmacies in a closed system and only for the treatment of diseases. The use of drugs of abuse outside of this very limited medical practice and their sale is illegal, punishable by the criminal law.
This well-established formulation of drug policy now is threatened by an alternative vision that treats drugs of abuse the way alcohol and tobacco are treated: through regulated production and sale to adults for legal use for any purpose. The campaign for this alternative drug policy begins with the legalization of marijuana but the stakes are far greater because it applies to all drugs of abuse and because there are enormous potential profits to be earned in this new marketplace. This move erases the sharp line between legal and illegal drugs. Erasing this line frustrates prevention and it opens the floodgates to widespread drug use.
Addiction Goes Up When Percent Usage Increases
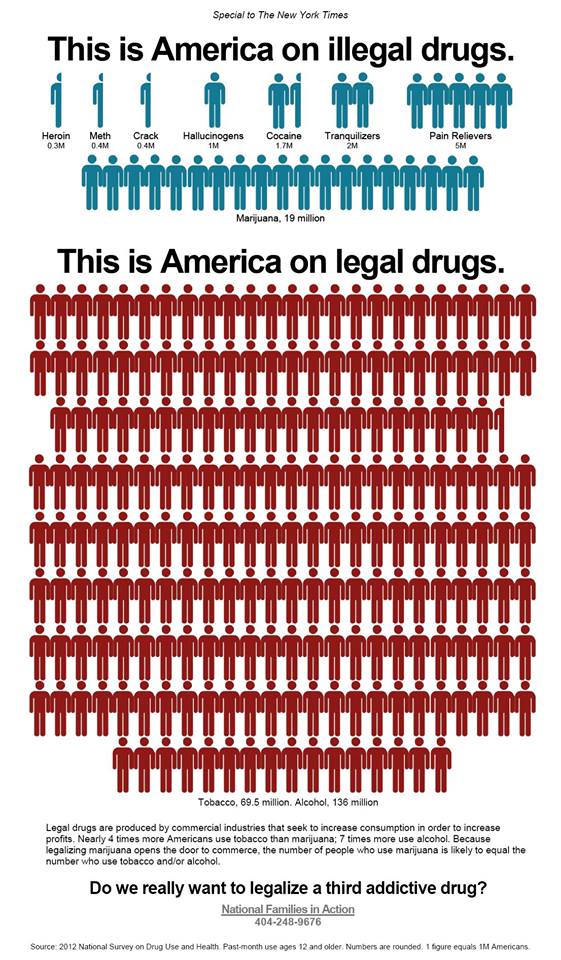
When considering the potential public health impact of the legalization of drugs of abuse, including marijuana, it is helpful to consider the rates of use of the two legal drugs. Among Americans age 12 and older, 52 percent used alcohol and 27 percent used tobacco in the past month whereas 9 percent used any illegal drug. Only 7 percent of Americans used marijuana. Treating marijuana – to say nothing of other drugs of abuse – the way alcohol and tobacco are treated most certainly will increase availability and with it dramatically increase the level of marijuana use to a level that is similar to the use of the two currently legal drugs.
Is increased marijuana use and subsequent proportional increases in marijuana addiction in the interest of the nation’s public health? I don’t think so. The use of alcohol and tobacco are the two leading causes of preventable illness and death in the United States. Adding a third legal drug will add to the devastation that these legal drugs already generate.
What is the better answer for the future of drug policy, if it is not the legalization and regulation of drugs of abuse? The future of an effective drug policy lies in finding ways to reduce the use of drugs of abuse that are compatible with modern values and laws. This search for better ways to reduce illegal drug use is the focus and the agenda of the Institute for Behavior and Heath, Inc. (www.ibhinc.org). There are many good new ideas for drug policy, all based on the recognition of the vulnerability of the brain to the excessive, unnatural stimulation of brain reward mechanism by drugs of abuse which leads to addiction for millions of people and the resulting devastation suffered by these individuals, their families and their communities.
Rather than embrace drug legalization, we must develop innovative policies and programs that reduce the use of drugs of abuse and we must provide assistance, including quality treatment that achieves long-term recovery, to those with substance use disorders.
Robert L. DuPont, M.D.
President, Institute for Behavior and Health, Inc.
Former Director, National Institute on Drug Abuse (1973-1978)
Former White House Drug Chief (1973-1977)
(Editor’s Note–Original article, “The Changing State of Drug Policy,” is reprinted with permission from the Institute of Behavior and Health website, where footnotes align exactly with text. It publishes several excellent articlesabout the influence of drug policy on addiction, drugged driving,etc.)
American Society of Addiction Medicine. (2011). Public Policy Statement: Definition of Addiction. Chevy Chase, MD: American Society of Addiction Medicine. Available: http://www.asam.org/advocacy/find-a-policy-statement/view-policy-statement/public-policy-statements/2011/12/15/the-definition-of-addiction
National Institute on Drug Abuse. (2010). Drugs, Brains and Behavior: The Science of Addiction. NIH Pub No. 10-5606. Rockville, MD: National Institute on Drug Abuse, National Institutes of Health, US Department of Health and Human Services. Available: http://www.drugabuse.gov/sites/default/files/sciofaddiction.pdf
Drug Enforcement Administration. (2014). The Dangers and Consequences of Marijuana Abuse. Washington, DC: Drug Enforcement Administration Demand Reduction Section, US Department of Justice. Available: http://www.justice.gov/dea/docs/dangers-consequences-marijuana-abuse.pdf
Manchikanti, L., Fellows, B., Ailinani, H., & Pampati, V. (2010). Therapeutic use, abuse, and nonmedical use of opioids: a ten-year perspective. Pain Physician, 13(5), 401-435. Available: http://www.painphysicianjournal.com/2010/september/2010;13;401-435.pdf
Centers for Disease Control and Prevention. (2014). Prescription Drug Overdose in the United States: Fact Sheet. Atlanta, GA: Centers for Disease Control and Prevention, National Center for Injury Prevention and Control, Division of Unintentional Injury Prevention. Available: http://www.cdc.gov/homeandrecreationalsafety/overdose/facts.html
Kuehn, B. M. (2014). Driven by prescription drug abuse, heroin use increases among suburban and rural whites. JAMA, 312(2), 118-119.
Johnson, K. (2014, April 17). Heroin is a growing threat across USA, police say. USA Today. Available: http://www.usatoday.com/story/news/nation/2014/04/16/heroin-overdose-addiction-threat/7785549/
National Institute on Drug Abuse. (2013, April). Heroin. DrugFacts. Rockville, MD: National Institute on Drug Abuse, National Institutes of Health, US Department of Health and Human Services. Available: http://www.drugabuse.gov/sites/default/files/drugfacts_heroin_final_0.pdf
Cicero, T. J., Ellis, M. S., Surratt, H. L., & Kurtz, S. P. (2014). The changing face of heroin use in the United States: a retrospective analysis of the past 50 years. JAMA Psychiatry, 71(7), 821-826.
Pew Research Center. (2014, April 2). America’s New Drug Policy Landscape. Washington, DC: Pew Research Center. Available: http://www.people-press.org/files/legacy-pdf/04-02-14%20Drug%20Policy%20Release.pdf
Volkow, N.D., Baler, R.D., Compton, W.M., & Weiss, S.R.B. (2014). Adverse health effects of marijuana use. The New England Journal of Medicine, 370(23), 2219-2227.
Richter, K. P., & Levy, S. (2014, June 11). Big marijuana—lessons from big tobacco [Perspective]. The New England Journal of Medicine. Available: http://www.nejm.org/doi/full/10.1056/NEJMp1406074
Substance Abuse and Mental Health Services Administration. (2013). Results from the 2012 National Survey on Drug Use and Health: Summary of National Findings, NSDUH Series H-46, HHS Publication No. (SMA) 13-4795. Rockville, MD: Substance Abuse and Mental Health Services Administration.
Established in 1978, the Institute for Behavior and Health, Inc. (IBH) is a 501(c)3 non-profit organization working to reduce illegal drug use through the power of good ideas. IBH websites include: www.ibhinc.org, www.StopDruggedDriving.org, www.PreventTeenDrugUse.org, and www.PreventionNotPunishment.org.
Editor’s Note: There is much misunderstanding about “medical” marijuana. National Families in Action explains when a controlled substance becomes medicine. NFIA has also published some helpful leaflet on the difference between marijuana and “medical” marijuana.
It’s hard to protect kids when the names of medical marijuana dispensaries are so enticing. The stores using “health,” “wellness,” “medicinal” and “candy” in their titles make pot very alluring. Imagine if a liquor store, tobacco store, or pharmacies did the same. (See our investigation into medi-pot dispensaries.)
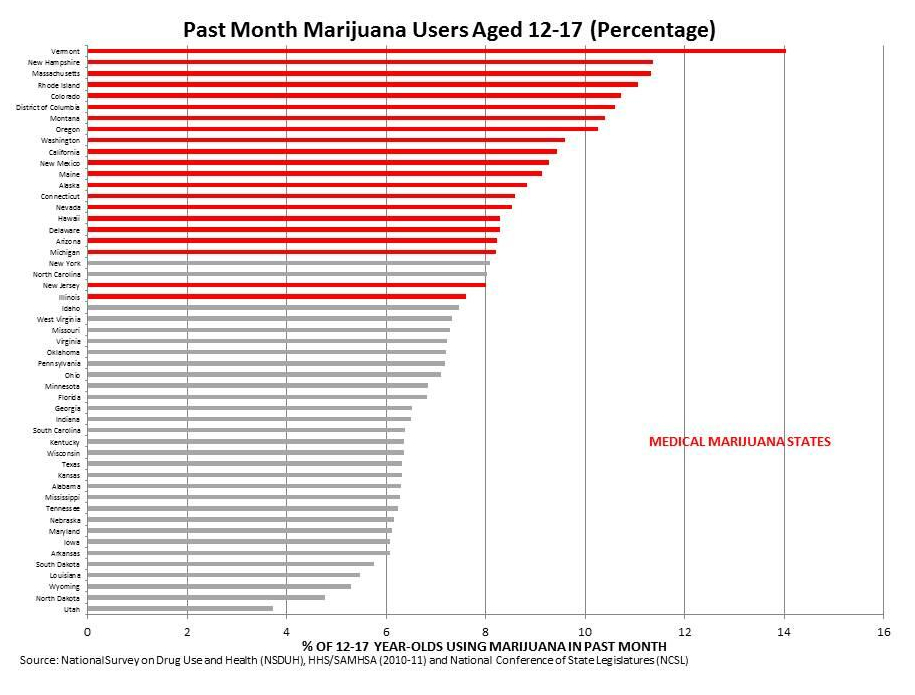
In states with medical marijuana, 12-17 year-old teens use marijuana to a much greater degree than in states without medical marijuana. States that voted down medical marijuana, Arkansas and South Dakota, have some of the lowest rates of youth marijuana usage. Before legalization in Colorado, a study showed that more than half the teen users surveyed said they had obtained pot from a medical marijuana ‘patient’.
Parents Opposed to Pot calls on those who support medical marijuana to address how to prevent substance abuse and secondary sales to children. The best laws have been adopted by state legislatures, as in New York and New Jersey. Whenever there have been statewide votes, as in California, Oregon, Washington, and Colorado, the records for protecting children are poor.
Teen usage has been going up since 1996, when medical marijuana was voted upon in the 1st state, California. Additionally, the teen perceptions of the risks in using marijuana have been going steadily downward since the 1991. Certain states with medical marijuana, especially Vermont, Oregon and Colorado, also have some of the highest usage of opiate pills, cocaine and alcohol in children and adults. It looks like marijuana is the gateway drug, when comparing state statistics for marijuana usage with all other drug usage. Vermont has been having a heroin problem this year, and Oregon has had problems with pill abuse over the past several years.
Testing and Approval of Drugs
As Americans have learned to expect easy, medicinal solutions to complex problems, the prescription drug and medical marijuana industries have grown.
While it is completely understandable that somebody that is sick, or the family of a patient, will want to use any means necessary to ease the pain and to cure, we would hope that there would be the correct information out there necessary to make a sound decision about the pros and cons of use.
Pharmaceutical drugs must undergo rigorous testing by the Food and Drug Administration (FDA) before approval. During these tests, placebos can work almost as well as the drugs being tested. Approved pharmaceutical drugs must warn of any and all potential side effects.
On the other hand, marijuana is recommended without warnings, and providers often do not need to prove their qualifications. Claims of cures by medical marijuana are promoted without testing. The marijuana plant holds 480 chemical components. If one component holds curative properties, another component could work against that property or have negative side effects.
Even if marijuana helps Multiple Sclerosis (MS), it also increases the brain fog in MS in patients. Why aren’t we discussing side effects when we talk medical marijuana? According to former Congressman Patrick Kennedy of Project SAM, the Institute of Medicine has concluded that if there is a future for marijuana as medicine, it lies in isolated components.
Epidiolex, a derivative of CBD in liquid form, is available to children with epilepsy in 10 states. It is being fast-tracked for FDA-approval, along with Sativex for Multiple Sclerosis. Sativex, a derivative of marijuana will be used for as a tongue spray. Both products were developed by GW Pharmaceuticals of Great Britain.
Conventional and Alternative Medicine
Getting a dog has been shown to be a very good solution for those who suffer from Post-Traumatic Stress-Syndrome (PTSD). Both yoga and dogs can bring back connectivity, open up energy and free blocked emotions. Quite the opposite could occur with use of marijuana. It may bring relief by numbing feelings even more, but it is known to harm memory and may not allow PTSD survivors a recovery back to their prior state of functioning.
There are problems with conventional treatments for cancer, but there are also problems with alternative treatments for cancer. The marijuana lobby has yet to explain why marijuana is often not the drug of choice for cancer patients in medical marijuana states. Is it because there are better drugs out there? Marinol, a synthetic marijuana, has been available to address the nausea and vomiting from cancer treatments and AIDs.
In Montana a few years ago, Cashy Hyde’s father claimed to have cured his son of cancer using cannabis oil. Sadly, the boy eventually died, after dramatic announcements that he had been cured. The constant nurture and love from his parents probably helped to extend his life. Any parent may have tried the same thing, maybe preferring it over harsh chemotherapy treatments.
When reading about the remarkable claims advocates of medical marijuana propose, please remember the placebo effect. We don’t know why placebos cure some people and not others. It could be the power of belief, or the result of a person’s own immune system having the ability to fight the disease.
Diet change can treat many of the autoimmune diseases which medical marijuana advocates list as conditions to be treated with marijuana: Crohn’s Disease, Rheumatoid Arthritis and Multiple Sclerosis. Medical marijuana treatments address the symptoms of disease, rather than the underlying causes. Diet and environmental changes can bring us closer to addressing the root causes of autism, autoimmune disease and epilepsy.
The ketogenic diet is a very successful means of controlling Dravet’s Syndrome and other types of epilepsy in children, a fact not discussed by those advancing medical marijuana.
Sometimes psychiatric medications are blamed for the actions of disturbed mass killers, such as Adam Lanza. However, James Holmes, Jared Loughner and Johar Tsarnaev were heavy marijuana users. Even the recent Santa Barbara killer, Elliot Rodger, had made a video about using marijuana every day.
We do not know the extent to which marijuana or pharmaceutical drugs contribute to teen violence. While the pharmaceutical industry has flaws, at least rigorous testing is required. The government has the ability to take a drug off the market.
Where’s the Expertise?
In this day and age, when people want miracles and pharmaceutical drugs can fall short of expectations, the marijuana industry looks for potential openings.
All claims of marvelous, miraculous cures need to be viewed with skepticism, whether considering pharmaceutical medicine or marijuana as medicine.
The push to reschedule marijuana from a schedule I to schedule II drug comes from Rick Doblin, the same person who wanted the FDA to approve MDMA (Ecstasy) as medicine. Doblin holds a PhD in Political Science. He doesn’t have the credentials you’d expect from someone making medical judgments.
The designation of marijuana as a Schedule I drug, meaning “high probability of abuse,” was upheld by the Federal Appeals Court for the DC Circuit, on January 22, 2013. Three pot advocacy groups had appealed a Food and Drug Administration (FDA) ruling of July 8, 2011, a ruling backed up by evidence by the Department of Health and Human Services. Previous reviews were in 1972 and 1986. Pot has become more potent since that time. There were 455,000 hospital emergency room visits for marijuana in 2011, a reason the FDA and Health and Human Services are reluctant to change.
The decision-making should come from the health and medical professions, using their expertise, not from political advocates.
Most doctors don’t agree with medical marijuana, but some see isolated components of the plant most helpful . The Pro-Con website lists 105 double-blind studies, and the conclusions from these studies are inconclusive: 40% suggest it can be helpful, 30% find no possible medical usage and 30% find it neither favorable or unfavorable.
If your state has a referendum, study the details. How does it protect children and prevent profiteering in the secondary markets?